Every year, millions of people reach for ibuprofen, naproxen, or celecoxib to ease joint pain, headaches, or backaches. These drugs work fast. But what most users don’t realize is that every pill carries hidden risks-risks that can quietly damage the stomach, kidneys, and even lead to life-threatening complications without warning.
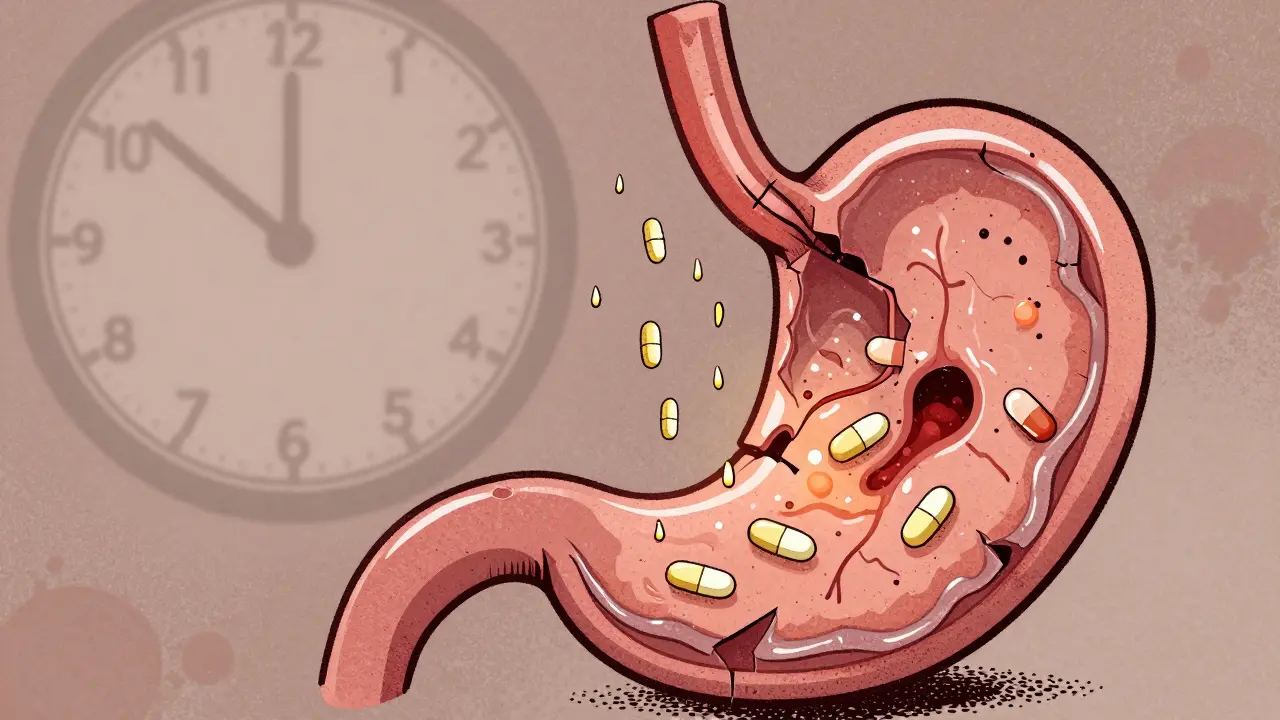
How NSAIDs Harm Your Stomach
NSAIDs don’t just block pain signals. They shut down protective chemicals in your gut called prostaglandins. These chemicals keep the stomach lining healthy by maintaining mucus production and blood flow. When they’re gone, your stomach lining becomes vulnerable. The result? Ulcers, bleeding, and perforations.Here’s the scary part: half of all NSAID-related stomach damage happens with no symptoms at all. You might feel fine, but inside, your stomach is slowly eroding. A 2021 study found that 15% of long-term NSAID users develop peptic ulcers. Some never know until they vomit blood or pass black, tarry stools-signs of internal bleeding.
It’s not just the upper GI tract. NSAIDs also attack the small and large intestines, causing inflammation, ulcers, and chronic diarrhea. Unlike stomach issues, there’s no reliable way to prevent or treat this lower GI damage. Even if you take a proton pump inhibitor (PPI) like omeprazole to protect your stomach, it won’t stop damage in your intestines. In fact, combining NSAIDs with PPIs for more than four months can increase your risk of microscopic colitis by over six times.
Kidney Damage: The Silent Threat
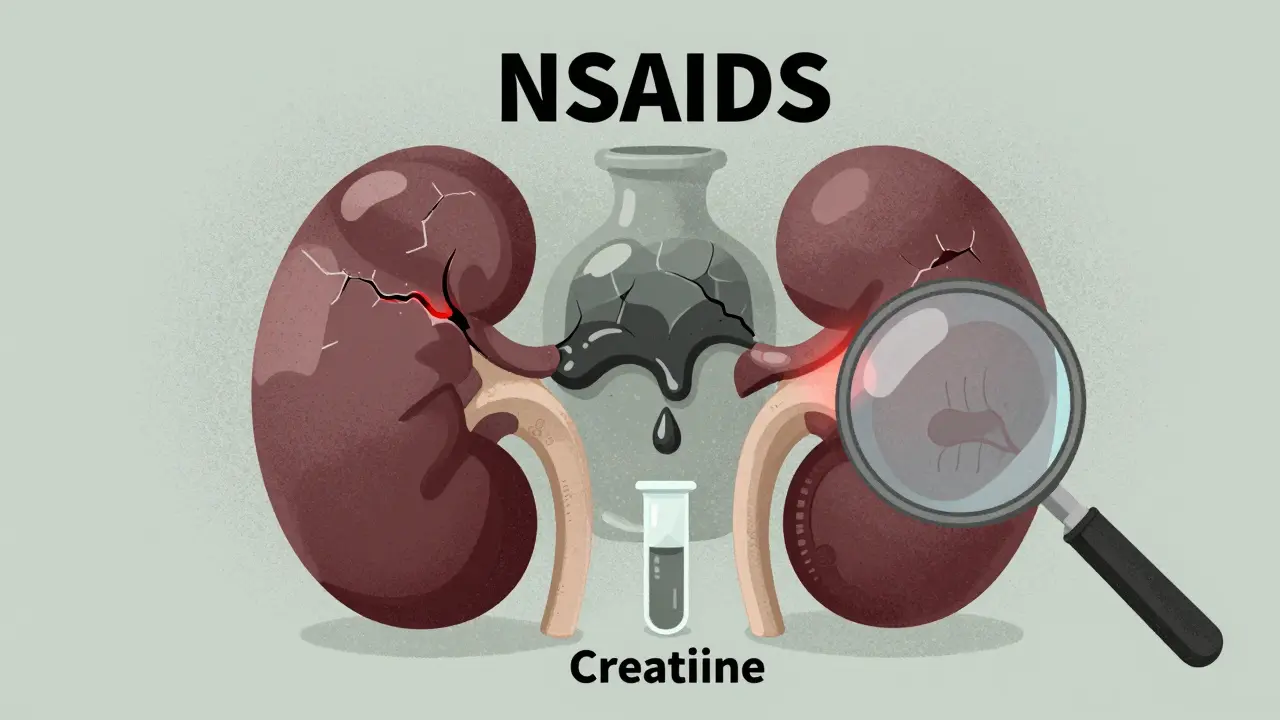
Your kidneys rely on prostaglandins to keep blood flowing through them, especially when you’re dehydrated or have high blood pressure. NSAIDs block those same chemicals. That means less blood gets to your kidneys, which can cause acute kidney injury-even in people who’ve never had kidney problems before.Studies show 1% to 5% of NSAID users develop sudden kidney failure. For older adults or those with existing kidney disease, that risk jumps dramatically. The FDA now requires a boxed warning on all prescription NSAIDs for patients over 65, citing the high chance of kidney damage. Long-term use can lead to chronic kidney disease, interstitial nephritis, or even papillary necrosis-a rare but severe condition where parts of the kidney tissue die.
What makes this worse? Many people don’t get their kidney function checked after starting NSAIDs. Only 52% of users have a creatinine test within 90 days, according to Medicare data. Without that simple blood test, kidney damage can go unnoticed until it’s advanced.
Who’s at Highest Risk?
Not everyone faces the same level of danger. Your risk goes up if you:- Are over 65
- Have had a stomach ulcer or bleeding before
- Take blood thinners like warfarin or aspirin
- Use corticosteroids (like prednisone)
- Have heart failure, high blood pressure, or kidney disease
- Take SSRIs (antidepressants), which raise bleeding risk by 3.4 times when combined with NSAIDs
The American College of Gastroenterology has a simple risk calculator. Add up points: age over 65 = 2 points, past ulcer = 3 points, blood thinners = 2 points. If you hit 4 or more, you’re high risk. That means you shouldn’t take NSAIDs without serious precautions.
Which NSAID Is Safest?
Not all NSAIDs are created equal. Naproxen carries the highest risk of stomach bleeding-4.2 times higher than non-users. Ibuprofen is nearly three times riskier than celecoxib. Celecoxib, a COX-2 inhibitor, is gentler on the stomach but still raises heart attack and stroke risk, especially in people with existing cardiovascular disease.Here’s what the data shows:
| NSAID | Relative Risk of GI Bleeding | Key Concerns |
|---|---|---|
| Naproxen | 4.2x | High GI risk, moderate CV risk |
| Ibuprofen | 2.7x | Common OTC use, frequent misuse |
| Celecoxib | 1.9x | Lower GI risk, higher CV risk |
| Aspirin (low-dose) | 1.5x | Used for heart protection, still causes GI bleeding |
There’s no perfect choice. Naproxen may be safer for the heart but harder on the gut. Celecoxib protects the stomach but isn’t safe for people with heart disease. The only real winner? Avoiding NSAIDs altogether when possible.
Monitoring: What You Need to Check
If you must take NSAIDs, you need to monitor. Not just when you feel bad-regularly, even if you feel fine.- Serum creatinine: Get tested within 30 days of starting, then every 3-6 months if you’re on it long-term.
- Blood urea nitrogen (BUN): Helps assess kidney function alongside creatinine.
- Complete blood count (CBC): Checks for anemia from hidden bleeding.
- Fecal occult blood test: Recommended every 6 months for high-risk users to catch silent GI bleeding.
Many doctors skip these tests. But in the Veterans Health Administration, pharmacist-led monitoring programs cut NSAID complications by 31%. Automated alerts in electronic health records help too. Don’t wait for your doctor to bring it up-ask for these tests.
What to Do Instead
The best way to avoid NSAID risks is to avoid NSAIDs. For chronic pain like osteoarthritis, try:- Physical therapy and strength training
- Topical diclofenac gel (much lower systemic absorption)
- Acetaminophen (paracetamol) for pain relief-no GI or kidney risk, but don’t exceed 3,000 mg/day
- Weight loss if overweight-every pound lost reduces knee stress by 4 pounds
- Heat/cold therapy, braces, or assistive devices
For acute pain-like a sprained ankle or headache-limit NSAIDs to 3-5 days. Never use them for more than 10 days without medical supervision. Each extra week of use increases your complication risk by 3-5%.
New Developments and What’s Coming
There’s some hope on the horizon. In 2023, the FDA approved naproxcinod, a new NSAID that releases nitric oxide to protect blood vessels and reduce ulcers by 58% compared to regular naproxen. In 2024, a new point-of-care fecal test became available that detects hidden bleeding with 92% accuracy-perfect for NSAID users who don’t show symptoms.But experts warn: without better ways to protect the lower GI tract, hospitalizations from NSAID damage could rise 18% over the next decade. Even the newest drugs won’t fix the core problem: we’re treating symptoms without addressing the root cause.
Final Advice: When to Stop
If you’ve been taking NSAIDs for more than a few weeks, ask yourself:- Do I still need them? Could I cut back or stop?
- Have I had my kidney function checked in the last 6 months?
- Do I have any signs of bleeding-dark stools, fatigue, dizziness?
- Am I taking a PPI? If so, for how long? More than 4 months? That might be doing more harm than good.
NSAIDs aren’t harmless. They’re powerful drugs with serious trade-offs. The goal isn’t to scare you off-just to make you aware. If you’re using them daily, you’re not just managing pain. You’re managing risk. And that risk deserves attention, not ignorance.
Can I take NSAIDs if I have high blood pressure?
NSAIDs can raise blood pressure and interfere with blood pressure medications. If you have hypertension, avoid NSAIDs unless your doctor approves them and monitors your BP closely. Ibuprofen and naproxen are especially risky. Acetaminophen is a safer pain reliever option.
Is it safe to take ibuprofen every day for arthritis?
No. Daily use increases your risk of stomach bleeding, kidney damage, and heart problems. Even low doses over months can cause harm. Talk to your doctor about alternatives like physical therapy, topical treatments, or switching to a COX-2 inhibitor with a PPI if absolutely necessary.
Do PPIs fully protect me from NSAID damage?
No. PPIs reduce stomach ulcers by 70-90%, but they don’t protect your intestines. Long-term use with NSAIDs can cause microscopic colitis and may mask symptoms of bleeding. Use PPIs only if you’re high risk, and only for the shortest time possible.
What are the signs of kidney damage from NSAIDs?
Early signs are often silent. Later signs include swelling in legs or ankles, fatigue, reduced urine output, nausea, confusion, or shortness of breath. The only reliable way to catch it early is through blood tests-creatinine and eGFR. Don’t wait for symptoms.
Are OTC NSAIDs safer than prescription ones?
No. OTC NSAIDs are the same drugs as prescription ones-just in lower doses. People often take them longer and more frequently than recommended. That’s why most NSAID-related hospitalizations come from OTC use. Never assume "over-the-counter" means "safe for long-term use."















Stephen Tulloch
Bro. I’ve been popping ibuprofen like Skittles since college. Now I’m 38 and my kidneys are whispering in Morse code. 🤯 Time to listen. Thanks for the wake-up call.